
Opioid epidemic continues to trouble Central Ohio physicians
* Thoughts from a Central Ohio physician
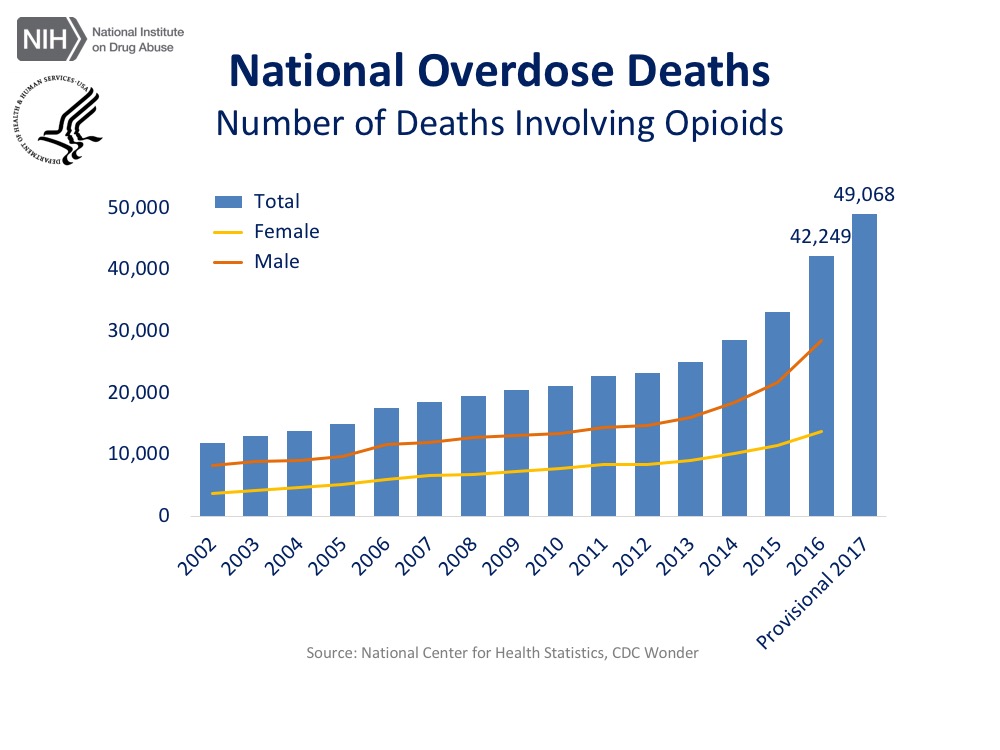
Recent news that the US life expectancy continues to decrease, in part due to an increase in unintentional deaths including from opioid overdose, is sobering (1). The US Centers for Disease Control reports 116 people died each day in 2016 from illicit or prescribed opioid overdose, and this number has increased to 134 based on preliminary data for 2017.
(Graphics provided by the NIH National Institute on Drug Abuse)
https://www.drugabuse.gov/related-topics/trends-statistics/overdose-death-rates
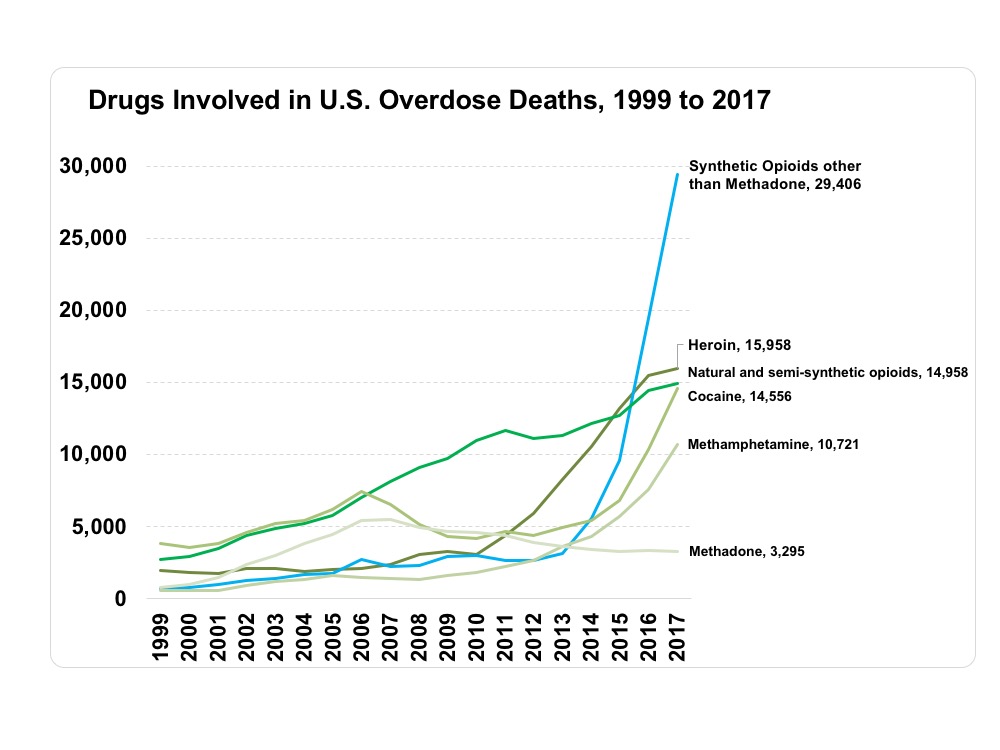
Ohio has not fared well in this epidemic; in 2016, Ohio had twice the national rate of opioid-related overdose deaths (32.9 per 100,000 persons compared to 13.3 per 100,000 persons) and an opioid prescription rate that was higher than national average (2). Synthetic opioids such as fentanyl have become less expensive and more prevalent, and now account for over half of opioid related overdose deaths in Ohio (2).

Graphic provided by the NIH National Institute on Drug Abuse: https://www.drugabuse.gov/drugs-abuse/opioids/opioid-summaries-by-state/ohio-opioid-summary
Morbidity associated with intravenous drug use has become a health crisis and poses significant costs to our health system. 9% of new HIV cases and 64% of new HCV cases diagnosed in 2015 were attributed to illicit intravenous drug use (IVDU) (2). Bacterial and fungal infections including endocarditis, osteomyelitis, bacteremia and abscesses associated with IVDU are common diagnoses on inpatient wards and require weeks of antibiotics and sometimes surgical intervention.
Data on these numbers is lacking, but one study through the University of North Carolina and North Carolina Department of Public Health found that rates of hospital admissions for IVDU associated endocarditis in North Carolina increased approximately twelvefold between 2010 and 2015, with sharper rates of increase in patients under 40 years old than in those older than 40 (3).During the same period of time, total hospitalization costs for IVDU related infectious endocarditis increased eighteenfold in North Carolina from $1.1 to $22.2 million (3).

In recent years, Ohio has implemented several beneficial strategies to combat the opioid epidemic. Expansion of Medicaid has significantly increased opportunity for medical care and addiction treatment for patients with opioid use disorder (OUD). Each year the state spends $1 billion in programs ranging from prevention education in pre-teen youth to sponsoring training sessions for medical providers to learn about prescribing medication assisted treatment (MAT) (Ohio MHAS). Establishing the Ohio Automated Rx Reporting System (OARRS) helps prescribers track patient prescription-shopping, and enforces association of opioid prescriptions with ICD codes. This limits the number of morphine equivalents and encourages providers to be thoughtful about prescribing.
Fortunately, there are multiple ways we, as medical providers, can help patients with OUD and prevent further addiction. Addiction medicine is not widely taught in medical school or training, but many educational tools are available to providers.
The American College of Physicians offers a free online CME course on safe opioid prescribing (ACP).The American Society of Addiction Medicine (ASAM) features many CME-accredited online courses and modules. ASAM sponsors DATA 2000 Suboxone waiver trainings around the state and online. These courses teach the physiology of opioid addiction, the pharmacology of MAT including buprenorphine, naltrexone and methadone, and allow for a provider to obtain a DEAX number, also known as a buprenorphine waiver.
Understanding that OUD is a chronic, relapsing disease just like diabetes or hypertension and that effective medications exist underscores that medical treatment is a core component of treating OUD. In patients with chronic opioid use, brain receptors have been altered and using is no longer a choice. Euphoria is rarely achieved, and thus patients continue to use opioids to prevent dysphoria and physical withdrawal. It often takes multiple attempts to quit before patients can achieve sobriety. As providers, our care and support as medical professionals and referrals for MAT helps patients to understand OUD as a chronic disease, and to feel that their life is worth saving.
In July, the Annals of Internal Medicine published a call to action recommending screening for OUD in all patients seen for overdose, new HIV or HCV infections, or bacterial and fungal infections related to IVDU (4). If patients screen positive, this call to action recommends immediate prescription of MAT and medications for withdrawal, and to find outpatient addiction treatment for these patients once they have been stabilized from their medical conditions (4).
In the clinic, questioning patients about OUD should be universal. Primary care providers who are waivered can prescribe MAT or can refer to local specialists. Partnering with social workers to find outpatient addiction resources for patients with OUD is crucial.
In Franklin County, Talbot Hall and Maryhaven are comprehensive substance use disorder treatment centers. The Substance Abuse and Mental Health Services website of the US Department of Health and Human Services provides an OUD treatment locator based on zip code for anywhere in the US (SAMHSA). Finally, as Medicaid is leading the way in paying for MAT and recovery programs, helping uninsured patients enroll in insurance programs will give them the best access to OUD treatment resources.
We as medical practitioners in central Ohio find ourselves at the heart of the opioid epidemic. Our state of Ohio and Medicaid are providing funds for collaborative evidence-based approaches to treatment and prevention of opioid use disorder. Through continuing education and partnering with local specialists and social workers, we can provide our patients the tools and support they need to achieve sobriety and rebuild their lives.
Margaret Williams, M.D. (Internal Medicine)
The Ohio State University Wexner Medical Center
Resources
“Mortality in the United States 2016, Centers for Disease Control,” https://www.cdc.gov/nchs/products/databriefs/db293.htm accessed 12/4/18
“Opioid summaries by state: Ohio”, NIH National Institute on Drug Abuse, www.drugabuse.gov, updated February 2018, accessed 12/4/18.
“Hospitalizations for Endocarditis and Associated Health Care Costs Among Persons with Diagnosed Drug Dependence — North Carolina, 2010–2015,” CDC Morbidity and Mortality Report Weekly, June 9, 2017 / 66(22);569–573”
Action Guide to Address Opioid Use, Governor’s Cabinet Action Team, May 2017 https://mha.ohio.gov/Portals/0/assets/Initiatives/GCOAT/GCOAT-Health-Resource-Toolkit.pdf accessed 12/4/18
SAFE opioid prescribing course, American College of Physicians: https://www.playbackacp.com/898?utm_source=REMS&utm_medium=ACPsite&utm_campaign=REMS accessed 12/4/18
American Society of Addiction Medicine educational learning center: https://www.asam.org/education accessed 12/4/18
US Department of Health and Human Services, SAMHSA MAT treatment locator: https://www.samhsa.gov/medication-assisted-treatment/physician-program-data/treatment-physician-locator accessed 12/4/18
Talbot Hall: https://wexnermedical.osu.edu/mental-behavioral/addiction-drugs accessed 12/4/18
Maryhaven: https://maryhaven.com/
“Effective Treatments for Opioid Addiction,” NIH National Institute on Drug Abuse, https://www.drugabuse.gov/publications/effective-treatments-opioid-addiction/effective-treatments-opioid-addiction accessed 12/4/18